
Minimally Invasive Treatments
Today, there are a number of minimally invasive treatment options that are covered by many insurance plans. While treatments like compression stockings are often first prescribed to manage symptoms, there are a variety of treatments that can actually treat the diseased veins to eliminate varicose veins, improve your quality of life and halt the progression of CVI.
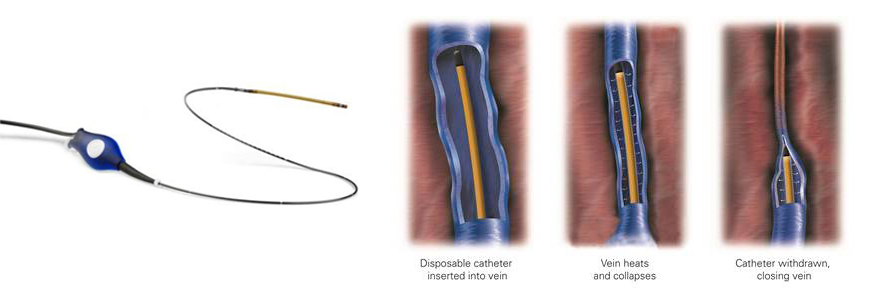
Endovenous Ablation
Endovenous thermal ablation is a minimally invasive treatment that involves the insertion of a thin, flexible tube called a catheter into a diseased vein to seal it shut using heat. Blood that would normally return toward the heart through these veins will then travel through other veins instead. Over time the treated vein shrinks and is absorbed by the body. Compared with surgical options like ligation and vein stripping, endovenous ablation results in less pain and quicker recovery time.
The ClosureFast™ radiofrequency ablation system, a clinically proven, minimally invasive treatment, seals problem veins for patients with CVI.
The Venefit™ procedure (VNUS closure) is the only minimally invasive segmental radiofrequency (RF) ablation treatment that utilizes radiofrequency energy to provide an even and uniform heat to contract the collagen in the vein walls, causing them to collapse and seal. Once a leg vein is closed, blood flow is redirected to healthy veins.
VNUS radiofrequency ablation allows for a quick, comfortable recovery and a return to everyday activities, while also improving the appearance of varicose veins.
The Venefit™ procedure is performed as a medical necessity to treat varicose veins as diagnosed by a trained vein specialist. For more information, visit: www.venefitprocedure.com

Experience the VenaSeal™ Closure System
The ClosureFast™ procedure is a minimally invasive treatment that uses radiofrequency (RF) energy to effectively treat
patients with varicose veins or chronic venous insufficiency (CVI). Because the valves in the legs cannot be repaired,
the only alternative is to re-route the blood flow from the diseased veins to the healthy veins.
To do this, a vein specialist inserts a catheter into the diseased vein through a tiny incision below the knee. Guided by
ultrasound imaging, a vein specialist will treat the vein in 7 cm segments for 20 seconds each. The catheter delivers
consistent and uniform heat to contract the collagen in the vein walls, causing them to collapse and close. After the
vein is sealed shut, blood is then naturally redirected to healthy veins. The treated vein then becomes fibrous tissue and
will gradually be absorbed into surrounding tissue.
How effective is the ClosureFast™ procedure?
The ClosureFast™ procedure has been shown in a large multicenter study to be 94.9% reflux-free at 5 years. Treating with the ClosureFast™ catheter resulted in high closure rates with improvements in CEAP Class grading and VCSS out to 5 years post treatment. The ClosureFastTM procedure has been shown in a large multicenter study to be 94.9% reflux-free at 5 years. The RECOVERY Study showed that patients experience less bruising and pain, and fewer complications with the ClosureFast™ procedure, using the Medtronic ClosureFast™ endovenous radiofrequency ablation (RFA) catheter in comparison to 980 nm laser ablation.
The ClosureFast™ procedure is performed as a medical necessity as diagnosed by a trained vein specialist. It is not designed to address spider veins or cosmetic issues. As with any medical procedure, you should consult a vein specialist and review all safety information associated with the procedure.
How is the ClosureFast™ procedure different from vein ligation and stripping?
Vein stripping is a surgical procedure. The surgeon makes an incision in your groin and ties off the vein, after which a “stripper” tool is threaded through the leg vein in order to pull it out through a second incision just above the calf. Bruising and swelling often occur post-procedure and nerve tissues surrounding the treated vein can be damaged, causing numbness or burning around the site.
The ClosureFast™ procedure is minimally invasive. In contrast to vein stripping, the vein remains in place and is closed using a special catheter inserted through a small incision below the knee. Vein stripping is usually performed in an operating room under a general anesthetic, while the ClosureFast™ procedure is often performed in an outpatient setting, typically using local or regional anesthesia.
How is the ClosureFast™ procedure different
from laser ablation?
The ClosureFast™ procedure utilizes radiofrequency energy to provide consistent and controlled heat to contract the collagen in the vein walls, causing them to collapse and seal. Once a leg vein is closed, blood flow is redirected to healthy veins. Laser ablation uses laser heat to collapse and seal the affected vein. The laser targets blood in the vein, causing it to heat. This heat creates a steam bubble inside the vein, causing damage to the vein so that it collapses. Unlike the ClosureFast™ procedure, laser temperatures can reach over 1200⁰C, which can lead to increased bruising and post-procedural pain for the patient. Animal studies have shown that laser can potentially lead to perforation and destruction of the vein walls13, causing significantly more bruising and post-procedure pain for patients (see next page for potential risks and/or complications associated with the ClosureFastTM
procedure).
The RECOVERY Study compared the experience of patients treated with the ClosureFast™ procedure and those treated with 980 nm laser ablation. The findings clearly demonstrated that the ClosureFast procedure resulted in less pain, less bruising, and fewer complications.
In the RECOVERY Study, the author concluded, “RF thermal ablation (ClosureFast™ procedure) was significantly superior to laser ablation as measured by a comprehensive array of postprocedural recovery and quality of life parameters in a randomized prospective comparison between these two thermal ablation modalities for closure of the Great Saphenous Vein.”
How long does the ClosureFast™ procedure take?
The ClosureFast™ procedure takes approximately 45-60 minutes. Most patients typically spend two to three hours at the medical facility due to normal pre- and post-treatment procedures.
Does the ClosureFast™ procedure require anesthesia?
The ClosureFast™ procedure can be performed under local, regional or general anesthesia. It is generally performed using local anesthesia in a vein specialist’s office or an outpatient surgical facility.
After the ClosureFast™ procedure, how quickly can I return to normal activities?
Many patients experience a quick return to normal activities, typically within a few days. For a few weeks following the treatment, a vein specialist may recommend a regular walking regimen and suggest you refrain from very strenuous activities (i.e., heavy lifting) or prolonged periods of standing.
How soon will my symptoms improve after the ClosureFast™ procedure?
Most patients report a noticeable improvement in their symptoms within one to two weeks following the procedure. For any cosmetic symptoms that are not completely resolved following the procedure, you may consider adjunctive treatment including sclerotherapy (small chemical injections) or micro phlebectomy (removal of varicose veins through small skin punctures under local anesthesia).
What potential risks and complications are associated with the ClosureFast™ procedure? Can I expect
any pain, bruising or tenderness after the ClosureFast™ procedure?
As with any medical intervention, potential risks and complications exist with the ClosureFast™ procedure. A vein specialist will have a consultation with you to determine if your conditions present any special risks. They will also review with you potential complications associated with the ClosureFast™ procedure, which can include but not limited to the following: adjacent nerve injury, hematoma, pulmonary embolism, thrombosis, infection, phlebitis, skin burn or discoloration, or vessel perforation. Patients report minimal to no scarring, bruising or swelling following the ClosureFast™ procedure.
Is the ClosureFast™ procedure suitable for everyone?
A vein specialist can tell you if the ClosureFast™ procedure is the right option for your vein problem. Experience has shown that many patients with chronic venous insufficiency can be treated with the ClosureFast™ procedure.
Is age an important consideration for the ClosureFast™ procedure?
The most important step in determining whether or not the ClosureFast™ procedure is appropriate for you is a complete ultrasound examination by a vein specialist. Age alone is not a factor in determining whether or not the ClosureFast™ procedure is appropriate for you. The ClosureFast™ procedure has been used to treat both women and men across a wide range of ages.
What happens to the treated vein left behind in the leg? Don’t I need it?
After treatment, the affected vein simply becomes fibrous tissue. Over time, the vein will be completely absorbed into surrounding tissue. Faulty valves interfere with the normal return of blood through the venous system. Closing these diseased veins helps to re-route the blood, improving circulation and relieving most symptoms.
Is the ClosureFast™ procedure covered by insurance?
Many insurance companies pay for the ClosureFast™ procedure in part or in full. The ClosureFast™ procedure has coverage policies with major health insurers. A vein specialist can discuss your insurance coverage further at the time of consultation.